No One Should Be Excluded from Health.
 Our collective health is getting better. In the last century, life expectancy in the US rose from 47 years to about 79 years. Notwithstanding recent, troubling declines in our national life expectancy, this overall trend is encouraging, and is due largely to improvements to the social, economic, and environmental context in which we live. Yet not everyone has shared in these gains. As we in public health well know, deep gaps exist between the overall health of populations and the health of vulnerable, marginalized groups.
Our collective health is getting better. In the last century, life expectancy in the US rose from 47 years to about 79 years. Notwithstanding recent, troubling declines in our national life expectancy, this overall trend is encouraging, and is due largely to improvements to the social, economic, and environmental context in which we live. Yet not everyone has shared in these gains. As we in public health well know, deep gaps exist between the overall health of populations and the health of vulnerable, marginalized groups.
The holidays, for all their cheer, are a time when these gaps can seem especially visible. It is not hard to find people enjoying the trappings of the season—rich food, expensive shopping, and all the other benefits that come with celebrating in a country that is, in general, quite well-off. Yet we can also see those who do not share the privileges of the majority—the many homeless, for example, who were the subject of last week’s note. Race, sexual orientation, gender identity, and economic status also too-often mark the boundary between those who are able to live healthy and those who are not. The challenges faced by marginalized groups are a reminder that health and wellbeing are not equally distributed in our society. In the middle of our “trilogy” of reflections on marginalized communities this holiday season, today’s note is a reminder that the work of building a better world is not done until the world is better for everyone—the few as well as the many.
A focus on the health of vulnerable groups within populations is a core remit of public health. This is well articulated in the mission of our School of Public Health: “To improve the health of local, national, and international populations, particularly the disadvantaged, underserved, and vulnerable, through excellence and innovation in education, research, and service.” Similar sentiments are echoed in the missions of other schools of public health worldwide. It is then not surprising to note that there is a substantial body of scholarship and research focused around health differences between populations, often characterized as health inequalities or health disparities research. Indeed, the body of work concerned with health disparities and health inequalities has been growing over the past 15 years, even as a proportion of total number of papers published annually has roughly plateaued.
否
It is reasonable, therefore, to ask: How are we doing on health inequalities? To what extent are we succeeding in narrowing health disparities between groups within the United States? I restrict my comments here to the US to narrow the scope of the conversation, although much of this could well be extended to other countries.
On some levels, particularly process indicators, we are indeed doing well.
One dimension that seems to be narrowing in disparities, at least among racial groups, is access to preventive care. Figure 1 below shows data from a CDC report that compares the proportion of children vaccinated for measles, mumps, and rubella. We can see a narrowing of the gap between white children and Hispanic and black children over time.
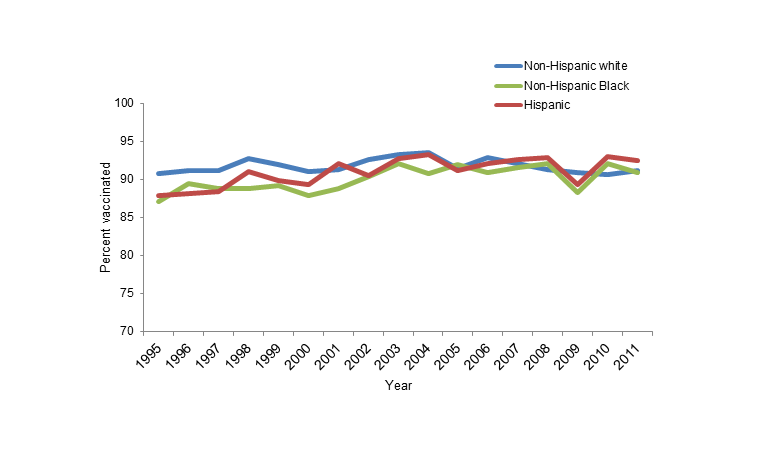
Figure 1. Estimated measles, mumps, and rubella (≥1 doses) vaccination coverage for children aged 19–35 months, National Immunization Survey, 1995–2011.
Another way of measuring preventive care is by looking at the proportion of adults who report having no usual source of health care, which has also narrowed over time across racial groups.
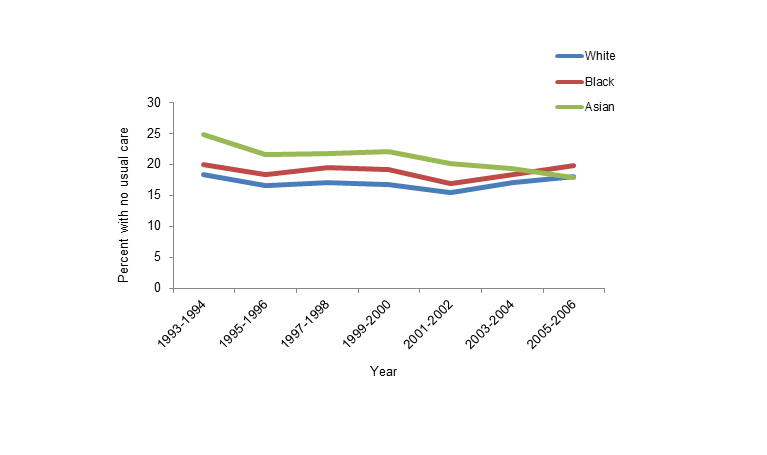
Figure 2. Percent of adults age 18–64 with no usual source of health care, 1993–2006.
Another good piece of news is that general public awareness of health disparities has improved. In a 1999 national survey, 55 percent of American adults said that they knew blacks and Latinos had poorer health outcomes than whites. In 2010, that number had increased to 59 percent. Although only a modest increase, and not as high as one might hope, it is perhaps heartening to know that as more policies and programs launch to try to narrow the gap, our general public is starting to understand, or at least recognize, disparities.
But, how are we doing on health indicators?
The final report for Healthy People 2010 reported on health disparities for 469 population-based health objectives, showing that although there was some improvement, disparities have either increased or stayed the same since baseline measures for the majority of objectives, particularly between racial and ethnic groups (see Figure 3).
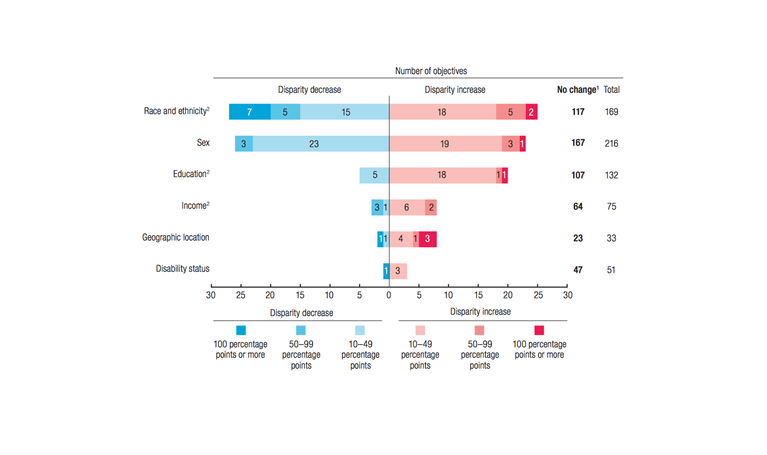
Figure 3. Changes in health disparities from baseline to most recent time points, Healthy People 2010.
One of the most basic measures of health disparities is life expectancy. From 2003 to 2013, we saw an increase in life expectancy for all race/gender groups (see Figure 4, below), and the gap between the white and black groups decreased slightly across years. However, there is still an astonishing 4.7-year difference among men and a 3.1-year difference among women between non-Hispanic white and black groups.
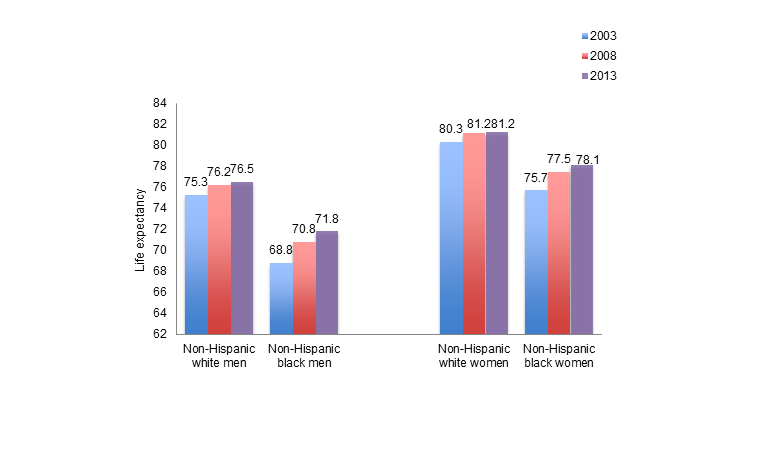
Figure 4. Life expectancy at birth in the US by race/ethnicity, 2003 and 2008.
Narrowing in on the top five causes of death in the US in 2010, we see that blacks have an elevated rate of all types of death compared to whites, with the exception of chronic lower respiratory diseases and accidents (see Figure 5).
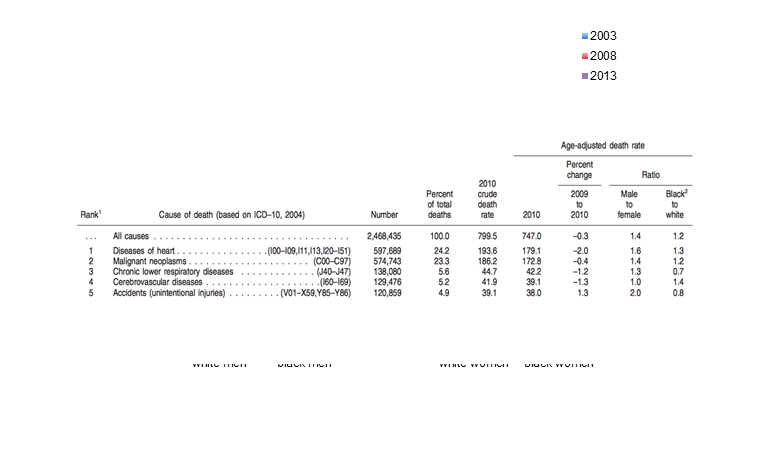
Figure 5. Death rates and ratios by cause of death for 2010, United States.
Disparities persist across a broad range of health indicators, visible not just by comparing death rates but also prevalence over time. This is clear with obesity, one of the most common chronic conditions in the US. Figure 6 below shows the prevalence of obesity among black and white women from 1976 to 2004. Black women have a higher level of obesity at every time point, and the gap remains wide throughout time, even increasing for the period of 2001 to 2004.
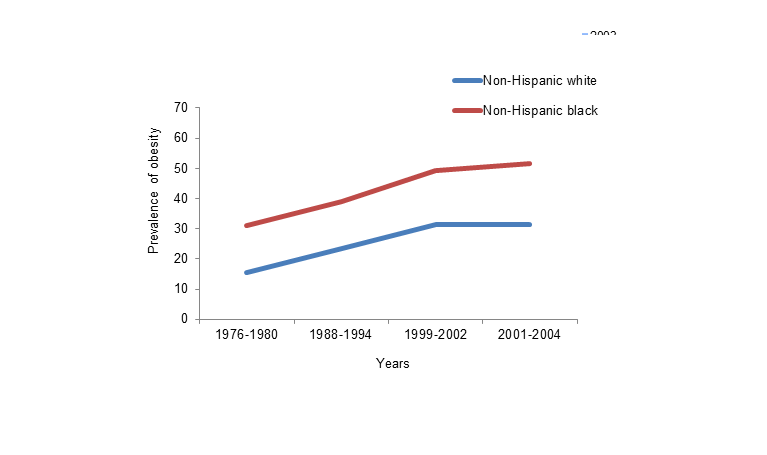
Figure 6. Age-adjusted prevalence of obesity among females age 20–74, 1976–2004.
Diabetes, another increasingly prevalent chronic condition in the United States, highlights racial and ethnic disparities as well. As can be seen in Figure 7, Hispanics, non-Hispanic blacks, and American Indians/Alaska Natives saw the highest proportions of adults with diagnosed diabetes from 2010 to 2012, with the prevalence among American Indians/Alaskan Natives at more than double that of non-Hispanic whites.
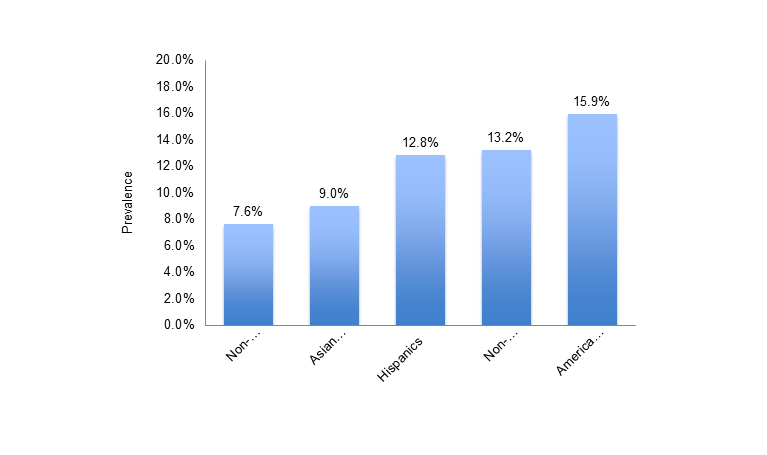
Centers for Disease Control and Prevention. National diabetes statistics report: Estimates of diabetes and its burden in the United States, 2014. Atlanta, GA: US Department of Health and Human Services; 2014. Available at: http://www.cdc.gov/diabetes/data/statistics/2014statisticsreport.html.
Figure 7. Age-adjusted prevalence of diagnosed diabetes among people 20 years old or older by race/ethnicity, 2010–2012.
Another example can be found in HIV and AIDS. The prevalence of HIV is greater among blacks than that among all other racial/ethnic groups, and black men have a higher proportion of HIV infections at all stages of the disease. Figure 8 shows estimated rates of HIV infection using the CDC’s national HIV surveillance system, and one can see that blacks have the highest rate and largest relative difference between groups in both 2005 and 2008.
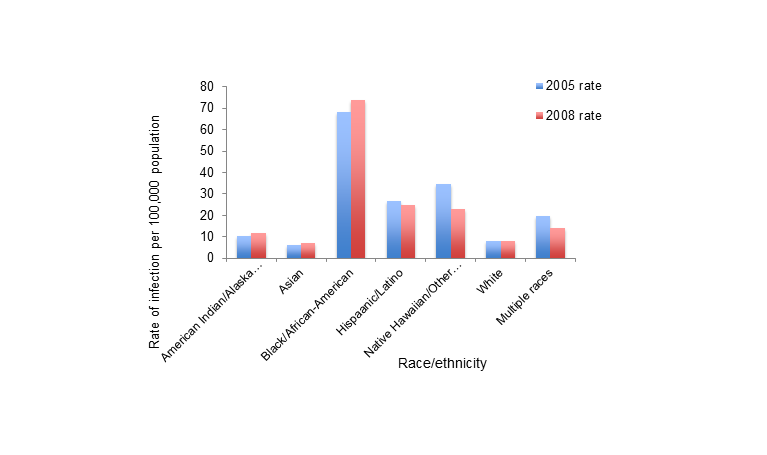
Created from Table 1 of Hall HI et al. HIV Infection—United States, 2005 and 2008. MMWR January 14, 2011. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/su6001a19.htm?s_cid=su6001a19_w.
Figure 8. Estimated rate of HIV infection diagnoses among persons aged ≥13 years—CDC’s national HIV surveillance system, 37 states, 2005 and 2008.
As a last example, we see a disparity between blacks and whites in terms of colorectal cancer incidence and deaths. In 2008, non-Hispanic blacks were 23 percent more likely than non-Hispanic whites to be diagnosed with colorectal cancer, and 46 percent more likely to die from it.
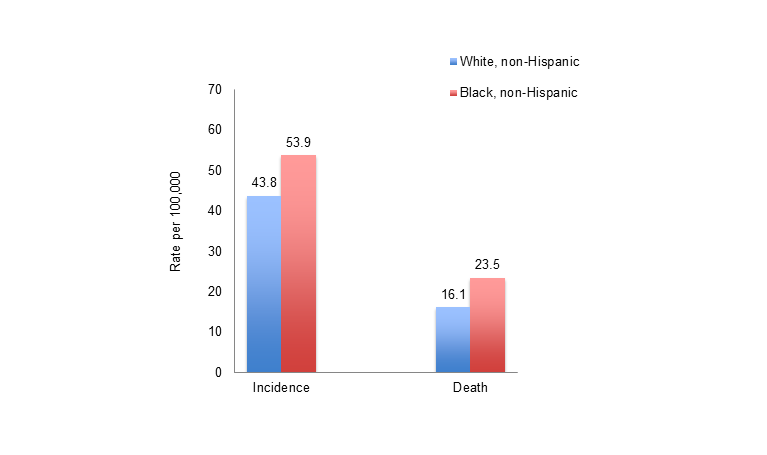
Figure 9. Age-adjusted incidence and mortality rates per 100,000 population from colorectal cancer by race/ethnicity, 2008.
Why do we have these persisting health inequalities despite substantial intellectual engagement with the issue, research spending in the area, and narrowing of access to care gaps?
μ

Figure 10. Adults under age 65 who were uninsured all year in 2005, by race, ethnicity, and language spoken at home.
At core, however, a more fundamental lens on the persistence of health inequalities is inescapably linked to deep and persistent economic inequalities between groups in the US.
US adults living at or below the federal poverty level are more than five times more likely to say they are in poor or fair health. The impact of economic disparities on health inequalities is pervasive, extending, for example, not only to differences between racial groups, but also to differences within racial groups. For example, black women are much more likely to have a sexually transmitted infection if they also had a lower education status, as shown in Figure 11 below.
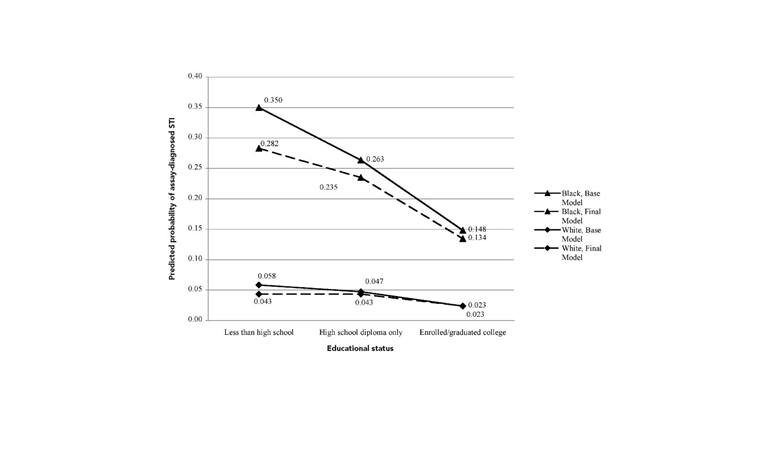
Figure 11. Probability of sexually transmitted infection by education.
电子商务
I hope everyone has a terrific week.
Warm regards,
Sandro
Sandro Galea, MD, DrPH
Dean and Robert A. Knox Professor
Boston University School of Public Health
Twitter: @sandrogalea
Acknowledgement. I would like to acknowledge the help of Laura Sampson and Eric DelGizzo with this Dean’s Note.
Previous Dean’s Notes are archived at: /sph/category/news/deans-notes/