The Determination of Health Across the Life Course and Across Levels of Influence.
 In the first part of this Dean’s Note, I suggested that a life course perspective can be a useful and essential organizing approach for population health science. I have, in previous work, suggested that life course approaches and multilevel approaches may be the two most important paradigmatic shifts in population health science in recent decades. Building then on the first part of this note, here I comment on multilevel approaches.
In the first part of this Dean’s Note, I suggested that a life course perspective can be a useful and essential organizing approach for population health science. I have, in previous work, suggested that life course approaches and multilevel approaches may be the two most important paradigmatic shifts in population health science in recent decades. Building then on the first part of this note, here I comment on multilevel approaches.
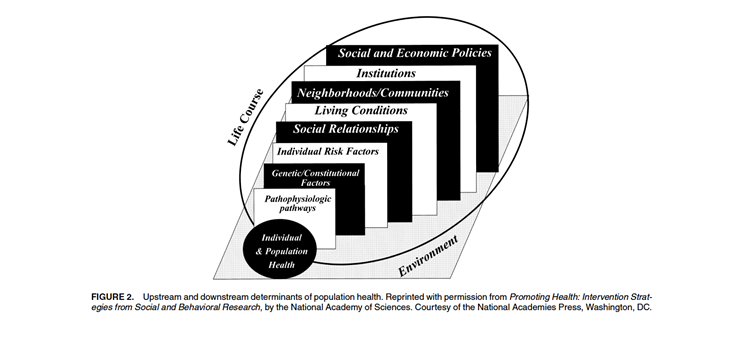
A multilevel approach to population health is predicated on the understanding that exposures at many levels of organization work together to produce health outcomes. These exposures are positioned both up and downstream of individual-level risk factors [see Figure 1] and include determinants of population health that are social, biological, geographic, political, and temporal in nature.
Kaplan GA. What’s wrong with social epidemiology and how can we make it better? Epidemiol Rev., 2004; 26: 124-35.
Therefore, a multilevel approach teaches us to ask how it is that social relationships produce health behaviors that in turn may result in pathophysiologic manifestations of disease. A multilevel question might ask what the consequences are of lifting a law requiring motorcycle helmet use on head injuries in a particular state. This, of course, is in contrast to a “single-level” question that rests on individual associations and that would ask what the relationship is between an individual wearing her helmet and her risk of head injury.
A multilevel framework provides us with an opportunity to ask questions that extend our analytic lens beyond individual experience to a fuller appreciation of the levels of influence that plausibly shape the health of populations, all to the end of understanding what might indeed matter most and what might be useful levers of influence in our goal to improve population health.
来
Importantly, multilevel perspectives do not simply “add” isolated “risk factors” at other levels of influence to our prediction models. Multilevel frameworks should allow us to examine the interface between levels and quantify interactions across levels, and there is an established literature on theoretic and statistical considerations in appropriately modeling clustered or nested observations (e.g. people within neighborhoods).
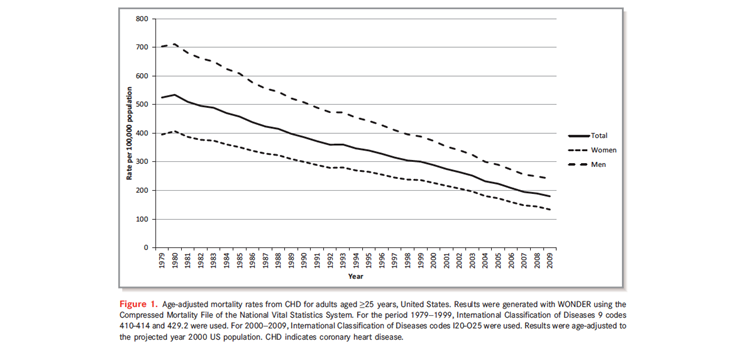
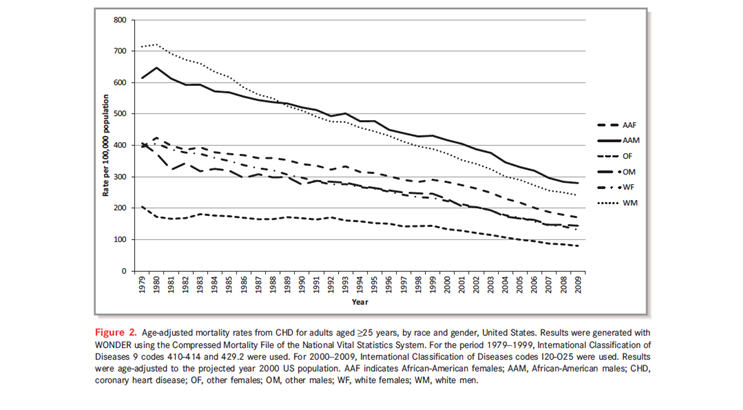
Extending the CHD example, from 1979 through 2009, CHD mortality declined by 66 percent among men and 67 percent among women [see Figure 2]. However, these general gains mask differences by race, which emerge clearly in Figure 3, showing that despite the overall reduction in CHD mortality, the rates for African American men and women remain disproportionately highest relative to other race/gender groupings.
Ford ES, Roger VL, Dunlay SM, Go AS, Rosamond WD. Challenges of ascertaining national trends in the incidence of coronary heart disease in the United States. J Am Heart Assoc., 2014; 3(6), e001097. http://www.ncbi.nlm.nih.gov/pubmed/25472744
Ford ES, Roger VL, Dunlay SM Go AS, Rosamond WD. Challenges of ascertaining national trends in the incidence of coronary heart disease in the United States. J Am Heart Assoc., 2014; 3(6), e001097. http://www.ncbi.nlm.nih.gov/pubmed/25472744
Why would this be?
Informed by a multilevel perspective, one could approach this question in a few ways. Can genomic differences explain racial disparities in CHD? Ample evidence suggests that genomic factors do not appear to explain racial disparities in population-level CHD burden. Could this difference be related to disparities in access to and quality of care? Perhaps, although the best available evidence suggests that disparities in access to and quality of care are likely to explain relatively little of these observed racial differences.
交货
This illustration demonstrates how an exploration of influences at multiple levels can shed light much more comprehensively on the determinants of population health than can a focus on single levels alone. This approach is rapidly gaining currency and broader acceptance. On the example of CHD, echoing this approach, the 2010 Institute of Medicine report “Promoting Cardiovascular Health in the Developing World” emphasized the need for a multilevel approach to CHD promotion [see Figure 4].

Institute of Medicine. Promoting cardiovascular health in the developing world: A critical challenge to achieve global health. http://www.iom.edu/Reports/2010/Promoting-Cardiovascular-Health-in-the-Developing-World-A-Critical-Challenge-to-Achieve-Global-Health.aspx. Released March 22, 2010.
Coming back then to life course and multilevel perspectives together, both approaches provide organizing principles that can guide our analytic and conceptual work in public health. Both can help frame the questions we ask and, hopefully, guide us to the production of more useful knowledge. And both, when put together, demonstrate the complexity of population health extending well beyond a deterministic approach that suggests a particular health behavior is the central factor responsible for health outcomes in populations. This clearly has implications for our scholarship, but also for our educational programs and for the practice of public health as a whole.
I hope everyone has a terrific week. Until next week.
Warm regards,
Sandro
Sandro Galea, MD, DrPH
Dean and Professor, Boston University School of Public Health
@sandrogalea
Acknowledgement. I would like to acknowledge the work of Gregory Cohen, MSW, on this Dean’s Note and the first Dean’s Note in this series.
Previous Dean’s Notes are archived at: /sph/category/news/deans-notes/